"mRNA has been studied in animals and it's safe it's not gene therapy the google facebook fact checked science said so!!"
First of all. The information here coupled with information given by experts in the field (in another post- experts not conspiracy theorists) coupled with my own health comorbidities (which have not been sampled for clinical trials) is enough to make me cautious on getting the vaccine, and I will probably wait 2 more years. The whole my body my choice reality also applies to forced medical treatment (other than the fact it is unconstitutional).
Search 'gene therapy' in the actual sec filing of these vaccines. Do your own independent research. It's important.
https://www.sec.gov/Archives/edgar/data/1682852/000168285220000017/mrna-20200630.htm
Here is another fact: serious adverse effects of gene altering treatments may not even be detected by short, minimal, small clinical trials, ESPECIALLY in highly biased clinical trials laden with conflicts of interest involving vaccine companies - ignoring this and allowing conflicts of interest for massive pharmaceutical companies but not in the usual standard of research is to live in a fantasy land. Let us not forget the sheer volume of money these companies make. Both Pfizer and AstraZeneca have an impressive track record of illegal activity.
A serious risk of coronavirus vaccines
A potentially fatal risk of coronavirus vaccines has been known for decades. It’s called antibody dependent enhancement (ADE). In simple terms, because of the way some viral antibodies work, they may actually backfire on the person when they subsequently encounter the wild virus. Non-neutralizing antibodies may enable the virus to enter the cells or the immune response may be skewed in other ways.
This is the reason why there has never been a coronavirus vaccine before. Often they tried developing coronavirus vaccines in the past, the test animals seemed to develop robust antibodies but when they were challenged with the wild virus, they got sick and died. This stopped the vaccine development in its tracks. This adverse reaction has been also seen with Dengue Virus, Ebola Virus, HIV, and RSV vaccines well. If there was a promising vaccine, it would have already been made.
The clinical trials for the Covid-19 vaccines2 were much too short to do proper and complete animal testing; the quick move to human trials, and to Emergency Use Authorization (not approval) of the vaccine, means that the global population will be used as the test animals in this experiment. The FDA, referring to it euphemistically as “vaccine-enhanced disease”, stated as much in their briefing document where they acknowledged that ADE will more likely be seen over time, following authorization or even after licensure, as vaccine immunity begins to wane.
Since ADE could potentially take months to years to occur in the various populations and demographics around the world, we may have a looming global disaster yet to come. One microbiologist has referred to it as a “ticking time bomb”.
Not only is this risk being ignored but, so too, is halacha (Jewish law).3
Here are the details:
FDA did not approve any vaccine for Covid-19
When the FDA issued an emergency use authorization (EUA) for the Pfizer vaccine (all other FDA authorized Covid-19 vaccines being rolled out now will only be for EUA), they specifically noted in their briefing document, albeit at the very end (were they trying to bury the problem?), that the potential for this was yet to be seen4 (emphasis added):
Available data do not indicate a risk of vaccine-enhanced disease, and conversely suggest effectiveness against severe disease within the available follow-up period. However, risk of vaccine-enhanced disease over time, potentially associated with waning immunity, remains unknown and needs to be evaluated further in ongoing clinical trials and in observational studies that could be conducted following authorization and/or licensure.
Since the FDA only gave authorization, not approval and licensure, for the vaccine, they emphasized that the Covid-19 vaccine is investigational in nature and people must be told the known and potential benefits and risks. and be given the right to refuse the vaccine (see image to right which is a slide introduced during their issuance meeting.5)
An agreement between the Israeli government and Pfizer, the full details of which are being withheld from the public, to roll out their vaccine to the entire Israeli citizenry6 is why, according to Pfizer CEO Albert Bourla: ‘Israel has become world’s lab right now’. 7 Unfortunately, the Israeli government is pressuring its citizens to take the vaccine, rather than giving them the option to refuse as per the FDA, and as is required under the Nuremberg Code written after the Holocaust to protect human beings from any future unwanted medical experimentation.
More than just a theoretical risk
An article in the International Journal of Clinical Practice8 raised concerns about the lack of informed consent for trial participants because of ADE.9 From the section entitled: “The Risk of ADE in COVID‐19 Vaccines is Non‐Theoretical and Compelling” (emphasis added):
Given past data on multiple SARS-CoV-1 and MERS-CoV vaccine efforts have failed due to ADE in animal models, it is reasonable to hypothesize a similar ADE risk for SARS-CoV-2 antibodies and vaccines. Here are a few papers.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5027702/
https://journals.asm.org/doi/full/10.1128/JVI.78.22.12672-12676.2004
https://www.nature.com/articles/s41564-020-00789-5
Former Pfizer scientists worried
Alarm bells were sounded by former Pfizer scientists Dr. Michael Yeadon, the ex-Pfizer head of respiratory research, and Dr. Wolfgang Wodarg, the lung specialist and former head of the public health department. They applied to the EMA, the European Medicine Agency responsible for EU-wide drug approval, to immediately suspend all SARS CoV 2 vaccine studies in human beings. The possibility of ADE, which needed to be studied better before the vaccine was introduced to the public, was one of the serious adverse events that they described when they filed their application.10
From the application (emphasis added):
A brief summary of their application can be found here.
There are many doctors and scientists, who have warned, and are warning about the dangers of Covid-19 vaccines. According to halacha, Shulchan Aruch (Orach Chaim, 618:4), when you have 2 doctors who say that there’s a risk of death, even if 100 doctors say there’s no risk, we listen to the 2 doctors. The Mishna Berurah explains: “ולא אזלינן בתר רב דעות בסכנת נפשות”(we do not follow the majority of opinions in a case of danger to life).
Is the vaccine a ticking time bomb?
Biochemist and molecular biologist, Dr. Doug Corrigan, believes it is.11 He explains that antibody dependent enhancement may not be seen for many years down the road:
Corrigan also raises another serious issue with Covid-19 vaccines. Since they are only designed to produce antibodies against one protein on the outer shell of the virus, they will only be protective against a single portion of the entire virus. He explains (emphasis added):
Getting the infection is much, much safer than getting the vaccine.
Disturbed by the way vaccine manufacturers disregard the dangers of ADE, he quotes from an article in Nature magazine (emphasis added):
And from the same article:
What would be the motivation for a vaccine manufacturer to throw caution to the wind and produce a vaccine that he knows can be worse than the illness it’s supposed to protect against? Can it be the fact that vaccine manufacturers have no liability, whatsoever, for any damage or deaths their Covid-19 vaccines may cause?12 According to halacha (Shulchan Aruch, Yoreah Deah 155:1), one is not allowed to use a doctor whose reputation and pocketbook are not at stake. Since none of the vaccine manufacturers or doctors recommending and/or administering the vaccine have any responsibility for deaths or injuries that may occur so their reputations and income will not be affected, taking this vaccine is prohibited.
Ignored warnings
The following video was uploaded on March 27, 2020. In it, Drs. Hotez and Offit, noted vaccinologists, discuss the dangers of rushing a coronavirus vaccine because of ADE. Offit says that he does not expect a coronavirus vaccine to be ready for stage 3 efficacy trials within 2 years. Yet, only 9 months later, first Pfizer, and then Moderna, received Emergency Use Authorization from the FDA, to, basically, conduct the rest of their stage 3 trials on the entire world.
https://www.youtube.com/watch?v=xCnOqwvPivE
Can ADE be avoided by repeat vaccinations?
The Israeli Prime Minister is betting on repeat vaccinations to avoid a potential disaster among the vaccinated (even as he’s still coercing everyone to vaccinate).
The People of Truth Association, in their appeal to the Israeli Supreme Court to stop human trials of the Pfizer Covid-19 vaccine, wrote that ADE was the reason that the Prime Minister has told those who vaccinated that they will need to keep vaccinating every six months.
Conclusion
Emergency use authorization is normally given16 when, among other considerations, the FDA commissioner believes that:
The FDA, despite knowing that a coronavirus vaccine has a real risk of killing many more people over time than Covid-19,17 went ahead and authorized the vaccine for emergency use. One must ask why, especially since CDC data shows that most people are not even in danger of dying from Covid-19.18’19
The FDA has not approved any remedies for Covid-19, such as hydroxychloroquine,20’21 Ivermectin,22 and others,23 which are well-known and inexpensive drugs that been shown to successfully treat Covid-19 and which could have saved thousands of lives. Since the existence of any alternative remedies would have meant that a (highly lucrative24) vaccine could not be authorized, they have not approved these remedies.
Furthermore, this is the first time in history that billions of people, adults and children alike, are expected to be inoculated (with a goal of inoculating every person in the world).
Data gathered from multiple countries already shows that this vaccine is injuring and killing people in great numbers shortly after they get it.25 Yet, just like the risk of ADE was not enough to stop the development and authorization of these vaccines, so too are the growing numbers of injuries not enough to put a halt to this program.
| ↑1 | https://upload.wikimedia.org/wikipedia/commons/thumb/2/20/Antibody-dependent_enhancement_%28ADE%29.png/1200px-Antibody-dependent_enhancement_%28ADE%29.png |
|---|---|
| ↑2 | Realistically, these should not be referred to as a vaccines. Vaccines contain either parts of the actual virus or a weakened or dead virus against which the body develops antibodies. These Covid-19 injections contain a synthesized version of the genetic coding (mRNA) for a part of the outer shell of the virus known as a spike protein. The mRNA, encapsulated in a lipid nanoparticle, finds its way into the cells and hijacks the cells machinery to translate the mRNA into the desired antigen, mimicking an infection to elicit an immune response. See https://www.rodefshalom613.org/2021/01/what-you-should-know-about-mrna-vaccines-clearly-explained/. (Some other vaccines will be using DNA and/or other technologies as means of entry into the cells.) |
| ↑3 | Rodef Shalom 613 has been wondering (see Rodef Shalom’s Response to Rabbi Lawrence Kelemen, footnote 9), even before any vaccine was introduced, why rabbanim haven’t been alarmed by the great religious destruction being caused to Jewish communities by government lockdowns and other measures. And now we have rabbanim who are encouraging their communities, and some even demanding that their congregants and students get vaccinated, even as numerous doctors and scientists warn against the vaccine, describing a number of mechanisms by which injuries and deaths are likely to occur in the mid-long term. Can those rabbis be causing a self-inflicted holocaust of epic proportions? |
| ↑4 | https://www.fda.gov/media/144245/download |
| ↑5 | https://youtu.be/owveMJBTc2I?t=2263 |
| ↑6 | Lawyer Valentina Nalin reviews the agreement between the Israel Ministry of Health and Pfizer here https://youtu.be/6n3sYfJr1Z8. Here is another review of the agreement https://rivkalevy.com/caught-in-the-lie-pfizer-and-the-ministry-of-health/ |
| ↑7 | https://www.israelnationalnews.com/News/News.aspx/297593 |
| ↑8 | https://onlinelibrary.wiley.com/doi/10.1111/ijcp.13795 |
| ↑9 | Note the difference between the adverse events listed in the EUA fact sheet to be given to recipients and caregivers, found at https://www.fda.gov/media/144414/download, as opposed to the EUA fact sheet for healthcare providers administering the injection, found at https://www.fda.gov/media/144413/download. Despite the more extensive listing for the providers, neither one mentions the risk of ADE or the 22 adverse events listed by The FDA Vaccines and Related Biological Products Advisory Committee October 22, 2020 Meeting Presentation as a draft “working list of possible adverse event outcomes” (https://www.fda.gov/media/143557/download, p. 17). They are (emphasis added): Guillain-Barré syndrome, Acute disseminated encephalomyelitis, Transverse myelitis, Encephalitis/myelitis/encephalomyelitis/meningoencephalitis/meningitis/encephalopathy, Convulsions/seizures, Stroke, Narcolepsy and cataplexy, Anaphylaxis, Acute myocardial infarction, Myocarditis/pericarditis, Autoimmune disease, Deaths, Pregnancy and birth outcomes, Other acute demyelinating diseases, Non-anaphylactic allergic reactions, Thrombocytopenia, Disseminated intravascular coagulation, Venous thromboembolism, Arthritis and arthralgia/joint pain, Kawasaki disease, Multisystem Inflammatory Syndrome in Children, and Vaccine enhanced disease. |
| ↑10 | https://2020news.de/wp-content/uploads/2020/12/Wodarg_Yeadon_EMA_Petition_Pfizer_Trial_FINAL_01DEC2020_EN_unsigned_with_Exhibits.pdf, p4 |
| ↑11 | https://sciencewithdrdoug.com/2020/08/01/is-a-coronavirus-vaccine-a-ticking-time-bomb/ |
| ↑12 | https://www.rt.com/news/496801-pharma-not-accountable-vaccine-effect/ |
| ↑13 | https://www.youtube.com/watch?v=xCnOqwvPivE&t=15s |
| ↑14 | They are also abandoning their placebo arm, allowing those who want, to receive the actual vaccine. This means that there may be no control group against which to measure the safety and effectiveness of the vaccine. https://www.chicagotribune.com/coronavirus/ct-life-covid-vaccine-placebo-pfizer-moderna-janssen-trial-20210114-r6vzmohbs5ed5gstqwuxdhtria-story.html The risk of that is compounded by the expected huge uptake of the vaccine among the global population, such as the situation that the Israeli government may be creating. |
| ↑15 | https://israel-news.co.il/archives/24886 |
| ↑16 | https://www.fdanews.com/ext/resources/files/archives/e/Emergency-Use-Authorization.pdf |
| ↑17 | Immune dysregulation is only one aspect of vaccine damage that can occur; there are likely to be many other serious adverse effects, as well. To learn more see http://enformtk.u-aizu.ac.jp/howard/gcep_dr_vanessa_schmidt_krueger/ |
| ↑18 | According to CDC data, the coronavirus survival rate is 99%-plus for for those 69 and younger, 94.6% for those who are older.https://www.breitbart.com/politics/2020/09/25/cdc-data-shows-high-virus-survival-rate-99-plus-for-ages-69-and-younger-94-6-for-older/ |
| ↑19 | Some scientists believe that another type of immune dysregulation may be more likely since antibodies are not the only determinants of immunity; other types of cells are also involved. In this scenario, faulty T-cells can trigger a serious outcome. Yet others are worried that the vaccines themselves will be responsible for mutations. See https://www.quantamagazine.org/how-vaccines-can-drive-pathogens-to-evolve-20180510/. |
| ↑20 | https://www.rodefshalom613.org/2020/09/about-medical-experts-and-consensus-in-light-of-the-hydroxychloroquine-debacle/ |
| ↑21 | http://www.c19study.com/ |
| ↑22 | https://www.cnsnews.com/article/national/susan-jones/physician-tells-senate-ivermectin-covid-wonder-drug-if-you-take-it-you |
| ↑23 | https://www.rodefshalom613.org/2020/08/the-treatment-of-viral-diseases-has-the-truth-been-suppressed-for-decades/ |
| ↑24 | https://www.chicagotribune.com/business/ct-biz-pfizer-covid-19-vaccine-profit-20210202-w3qkwajabfhsfk6i2gzihmlos4-story.html |
| ↑25 | https://drive.google.com/file/d/1gVLI6Y6e5mDfu0_7qc0Ozw1GkM69-CIC/view |
Despite the fact this mRNA technology has never been trialled on a large scale population of humans before, never on children under 18, never on pregnant women, and never on the older subset population they claim to care so much about, and existing studies are extremely limited, and that this should at least give some weariness...And not to mention the matter of record that both Pfizer and AstraZeneca are corporate criminals, having racked up billions in penalties over the last two decades for a host of dishonesty offenses including fraud, bribery and false marketing... The mRNA safety argument is false and misleading, and begs the question of where this information is coming from. It is apparent that a very minute amount of information are doing their own, unbiased research into real, significant, clinical trials, and I would have to say this is irresponsible.
The world is now being asked to forgive and forget the serial criminal dishonesty of these two pharma giants, and allow themselves to be injected with their poorly tested vaccines.
But what about Moderna? While most people know of Pfizer and AstraZeneca, many knew nothing of Moderna until it seemingly popped out of nowhere to become one of the main players in the COVID vaccine race.
The mRNA COVID-19 'vaccines' from Moderna and Pfizer-BioNTech are not really vaccines, at least not in the traditional sense. Instead, they are gene-modifying agents that insert synthetic messenger RNA into your cells. This synthetic mRNA contains instructions for your cells to produce a protein resembling the spike protein found on the exterior surface of a COVID-19 molecule. Your cells then eject this protein. Once outside the cells, it triggers the production of COVID-19 antibodies.
These antibodies will supposedly protect you against the 'deadly' COVID-19 which, as repeated studies have shown, is not very deadly at all. Even the CDC acknowledges the very low infection fatality rate (IFR) of COVID-19. Its best guess estimates show the only group where the IFR exceeds 0.5% is in the over 70s. In every other group, the IFR becomes a non-event, especially when compared with far more serious threats like cardiovascular disease, cancer, traffic accidents, drug and alcohol abuse, and suicide.
Table 1. Parameter Values that vary among the five COVID-19 Pandemic Planning Scenarios.
https://www.cdc.gov/coronavirus/2019-ncov/hcp/planning-scenarios.html
The early pioneer of mRNA technology was Hungarian-born scientist Katalin Karikó, who is now Senior Vice President at BioNTech. Driven by a belief in the revolutionary potential of mRNA technology to treat a host of diseases, she persevered with mRNA research despite a continual string of disappointing results. The enduring monkey wrench was that injecting synthetic mRNA routinely caused an unwanted immune response; the body sensed a foreign intruder and went into attack mode. The culprit was narrowed to one of the altered, synthetic RNA nucleosides which seemed to be triggering the immune system. Karikó and her Penn State colleague Drew Weissman swapped it out for a slightly modified version, creating a hybrid mRNA that could seemingly sneak its way into cells without alerting the body’s defenses. Well, at least under their experimental lab conditions.
This discovery was first published in 2005 and while it generally raised little fanfare, it did catch the attention of one Derrick Rossi at the Harvard Stem Cell Institute and Harvard Medical School. Rossi and his team experimented with the technology in his Harvard lab, and the researcher concluded he was on to something big. But with no entreprenurial experience, he needed advice. So he turned to Harvard colleague Tim Springer, who had been successful in taking his discoveries to market.
This led to an appointment with Bob Langer, a prolific MIT scientist and entrepreneur. Langer liked what he heard. So too did Noubar Afeyan, who the duo approached for funding. Afeyan was the CEO of Flagship Ventures, a venture capital firm investing in biotech start-ups.
The next big name on board was Ken Chien, a physician-researcher at Harvard and Sweden's Karolinska Institute, known for his work on heart stem cells. For years, Chien had been trying to figure out how to effectively regenerate heart muscle and vessels damaged by heart attack, and Rossi’s technology offered him a potential solution. He wanted in.
Rossi, Langer, Afeyan, and Chien banded together and in September 2010 announced the formation of Moderna. The following year, Stephane Bancel was lured from French diagnostics company BioMérieux to become Moderna's first CEO.
It's also worth mentioning that in 2017, a certain Moncef Slaoui joined Moderna's board of directors, after leaving his job at GlaxoSmithKline. Prior to joining the Moderna board, Slaoui had worked at GSK for some thirty years, starting as a vaccine researcher before being appointed head of research and development. Slaoui's name will resurface later in this story, under circumstances that hardly inspire confidence in the impartiality and independence of government health agencies.
The hyperbole from the new company came thick and fast, and investors piled in, hoping to catch a ride aboard the next Genentech. “We’re going to rewrite the book of biotech on this company," claimed the exuberant Bancel. "Everything’s going to be different. We’ll do nothing by the playbook.”
“It’s the perfect personalized medicine,” Bancel added. “You make your own drug.”
But the research results never lived up to the outlandish PR. When journalist Catherine Elton watched a Moderna scientist 'successfully' toy with modified mRNA in a lab experiment, Moderna’s chief scientific officer, Tony de Fougerolles, patted the scientist on the back, then told Elton, “In five years, that mRNA you just saw there might treat a disease that is currently not druggable.”
That was back in 2013.
Five years later, Moderna was still desperately trying to produce a viable mRNA drug. In fact, until the rushed "emergency authorization" of Moderna's mRNA COVID drug in December 2020, the company was nowhere close to successfully developing a single, approvable drug.
It wasn't for lack of trying.
By early 2013, Moderna had already filed 90 patent applications containing more than 4,500 claims.
In March 2013, Moderna and AstraZeneca signed a five-year agreement to discover, develop, and commercialize mRNA therapies for cardiovascular, metabolic, and kidney diseases, and even cancer. The agreement included a $240 million upfront payment to Moderna, a payment that was "one of the largest ever initial payments in a pharmaceutical industry licensing deal that does not involve a drug already being tested in clinical trials", and an 8% share in Moderna.
As of April 2020, only one candidate from the Moderna-AstraZeneca collaboration had even passed Phase I trials, the earliest stage of human research for drugs hoping to one day make it to market. The drug was a treatment for myocardial ischemia, labelled AZD8601.
In fact, right before winning federal funding for COVID vaccine development in March 2020, only 3 of Moderna's projects had made it past Phase 1 testing, and only one of these was a vaccine (a cytomegalovirus vaccine codenamed mRNA-1647).
In January 2014, Moderna and Alexion Pharmaceuticals entered a $125 million to develop rare orphan disease treatments, using Moderna's mRNA technology. However, by 2016, the program had been scrapped as animal trials showed Moderna's treatment would never be safe enough for use in humans.
In February 2016, an op-ed in Nature criticized Moderna for not publishing any peer-reviewed papers on its technology, and compared its secretive approach to that of the controversially failed Theranos.
In September 2018, Thrillist published an article titled, "Why This Secretive Tech Start-Up Could Be The Next Theranos", criticizing Moderna's secrecy and lack of scientific validation of its research. Noting the parallels with Theranos, Thrillist said Moderna "keeps investors in the dark," having "published no data supporting its vaunted technology ... Outside venture capitalists said Moderna has so many investors clamoring to get in that it can afford to turn away any who ask too many questions. Some small players have been given only a peek at Moderna's data before committing millions to the company."
Like Elizabeth Holmes, the eccentric CEO of the scandalized Theranos, Bancel is not a scientist. Said Thrillist, "his qualifications to make major scientific decisions at Moderna are also questionable ... Bancel had no experience running a drug development operation ... he'd spent most of his career in sales and operations, not science ... He is listed as a co-inventor on more than 100 of Moderna's early patent applications, unusual for a CEO who is not a PhD scientist."
Thrillist also succinctly summed up the problems with Moderna's supposedly world-changing technology. "The mRNA treatments it's trying to develop are potentially very dangerous ... Theoretically, the revolutionary treatments could target and reprogram specific cells, allowing our own bodies to cure themselves of disease with repeated doses over time."
But, as Thrillist noted, "A number of Big Pharma companies have attempted to develop similar technologies, but abandoned them over fear that they produced prohibitively dangerous patient side effects. Delivery - actually getting RNA into cells - has long bedeviled the whole field. On their own, RNA molecules have a hard time reaching their targets. They work better if they're wrapped up in a delivery mechanism, such as nanoparticles made of lipids. But those nanoparticles can lead to dangerous side effects, especially if a patient has to take repeated doses over months or years."
Indeed, severe allergy-like reactions occurred in at least eight people who received the Pfizer-BioNTech vaccine during a 2-week period after the vaccine rollout in December 2020. Like the Moderna vaccine, the Pfizer-BioNTech coats its synthetic mRNA with liposomes and a chemical called polyethylene glycol (PEG). PEG has never been used before in an approved vaccine, but is found in many drugs that have triggered anaphylaxis — a potentially life-threatening reaction that can cause rashes, plummeting blood pressure, shortness of breath, and rapid heartbeat. Fauci's NIH National Institute of Allergy and Infectious Diseases (NIAID) scrambled to convene several meetings to discuss the allergic reactions with representatives of Pfizer and Moderna, independent scientists and physicians, and the FDA. Little has since been said about the problem, even though adverse event reports from the vaccines continue to mount at a worrying rate. Instead, the public is being fed the brazen lie that the mRNA vaccines have been thoroughly tested and proven Safe and Effective!™
Moderna's Toxic Work Culture and High Staff Turnover
A 2016 STAT investigation found the company’s "caustic work environment has for years driven away top talent and that behind its obsession with secrecy, there are signs Moderna has run into roadblocks with its most ambitious projects." STAT interviews with more than twenty current and former employees and associates "suggest Bancel has hampered progress at Moderna because of his ego, his need to assert control and his impatience with the setbacks that are an inevitable part of science."
Former employees said they felt the business-minded Bancel prized the company’s ever-increasing stock market valuation over its science. As he pursued a "complex and risky" drug development strategy, Bancel built a culture of recrimination at Moderna, they said. Failed experiments were met with reprimands and even on-the-spot firings. They recalled abusive emails, dressings down at company meetings, exceedingly long hours, and unexplained terminations.
Others didn't wait around to suffer the full weight of Bancel's wrath. At least a dozen highly placed executives had quit in the previous four years, including heads of finance, technology, manufacturing, and science. In the twelve months prior to the STAT story, two respected scientists leading Moderna’s cancer and rare disease programs resigned, even though the company’s remarkable fundraising success had put ample resources at their disposal. Each had been at the company less than 18 months.
Even co-founder Rossi, whose vision was the initial seed for Moderna's formation, headed for the exit in 2014 as a result of internal squabbling.
Lower-ranking employees, meanwhile, said they were disappointed and confused by Moderna’s pivot to less ambitious — and less transformative — treatments. Despite boasting of world-changing technology that would one day cure the likes of cancer and heart disease, Moderna had switched its focus to vaccines.
While this change of course may have perplexed lower-ranking employees, there was actually a simple explanation.
Behind the scenes, the company’s scientists were running into a familiar problem. In animal studies, the ideal dose of their leading mRNA drug was triggering dangerous immune reactions — the kind for which Karikó and Weissman had supposedly improvised a workaround. A lower dose had proved too weak to show any benefits. If repeated doses of mRNA were too toxic to test in human beings, the company would have to rely on something requiring only one or two injections to show an effect. And so Moderna put its stable of experimental drugs on the backburner and morphed into a vaccines company.
Money Talks. Sadly, So Does Bullshit
Moderna sounds more reminiscent of Enron than the next Genentech. But while the company was repeatedly coming up short in the quest to make a viable mRNA drug, it sure knew how to whip investors into a frenzy with its lavish promises of world-changing therapies. When Moderna went public in December 2018, it was the largest biotech initial public offering in history, raising over $600 million on NASDAQ, and implying an overall valuation of $7.5 billion for the entire company.
As of this writing, the company currently enjoys a market capitalization of $71 billion. As some of the more grounded market analysts have noted, this absurd valuation is not justified by the underlying fundamentals. The US is unquestionably Moderna's biggest market. But even if the company sold the two-shot vaccine to every single American at the government-agreed price of $15 per dose, this would only equate to $9.2 billion in sales (not profit). For a company with no other presently viable drugs, a $71 billion market cap is insane.
Which might help explain the massive insider selling that has been taking place at Moderna. The company's CEOs have been dumping Moderna shares like bad smells at a whole-grain eating contest.
So the question is, how did an overhyped, overvalued company with absolutely no track record of successful drug production achieve something many older, established companies failed to do? Namely, become one of the very first companies to win "emergency use authorization" for a COVID-19 'vaccine'?
With government help and taxpayer money, of course.
The White House Version of 'Shark Tank'
One of the most oft-repeated criticisms leveled at former President Trump is his "mishandling" of the COVID-19 'crisis.'
Trump did indeed screw the pooch with his response to COVID-19, but not in the way sufferers of Trump Derangement Syndrome would have you believe. Right from the word go, everything about the official COVID story reeked of unbridled bullshit. We were told the virus emanated from a wet market in Wuhan, China, even though many of the initial patients - including the the first identified case - had no link to the market. We were told the virus 'jumped' to humans by a mythical feat of 'zoonotic transfer' after someone allegedly ate an infected bat ... no wait, it might have been a pangolin ... hang on, maybe it was a snake ... purchased from the market.
While there was never a shred of evidence to support this nonsensical claim, it is an established fact that a NIH-funded BSL-4 lab in Wuhan was deliberately creating virulent hybrid strains of bat coronaviruses. However, those who pointed out this inconvenient fact were quickly shouted down as "conspiracists," while the ridiculous wet market tale was embraced as the official mainstream origin story.
Then there was the tsunami of hysteria portraying the virus as humankind's Day of Reckoning. The virus was so contagious and so deadly, we were told, it mandated a new anti-social world order of physical ('social') distancing, mask-wearing and inhumane lockdowns. All the while, study after study showed that the virus had an infection fatality rate that could be measured in fractions of a percent.
To scare people into submission as a result of this otherwise weak virus, the complicit media needed a rapidly-increasing death count. An especially brazen and open admission the whole thing was an overblown sham came at a 7 April 2020 Whitehouse press briefing. After Trump handed the microphone over to Coronavirus Task Force member Joanne Birx, she nonchalantly admitted the US had taken a very "liberal" approach to counting COVID deaths. So liberal, in fact, that any death accompanied by a positive COVID result would be listed as a COVID death - even when the real cause of death was heart attack or kidney failure!
When a journalist queried this approach, Birx fumbled, leading Fauci to take the mike and confirm the alarming revelation that had just spilled from Birx mouth. This should have bought the whole charade to a crashing halt, as it confirmed the official COVID death count was a blatant fraud. The press of course, has long since proven it is a propaganda arm of the global elite, rather than a vector of factual information. But Trump was sitting there and, unless he was daydreaming about golf or reminiscing about one of his more memorable Miss Universe conquests, should have heard what Birx and Fauci just admitted to.
This is where Trump really screwed up on COVID-19. Instead of decisively calling bullshit on what was clearly a sham perpetuated by the same class of Deep State, swamp-dwelling malevolents he promised to chase out of town, he ended up buying into it. He should have immediately fired pseudoscientists like Birx and Fauci from his Coronavirus Task Force, and instead appointed scientists who promised not to count fatal heart attacks and kidney failure as COVID deaths. Instead, he let them remain. Not only did this ensure the perpetuation of a fraudulent COVID death count, where authorities even felt uninhibited about counting murder-suicides by firearm as COVID deaths, it guaranteed the brazen BS and fear-generation campaign would continue unabated.
Granted, Trump may not have embraced the COVID sham with the vigor of his clearly sociopathic Democrat opponents - he did ignore calls to keep US borders closed to travellers, and when he himself contracted COVID-19, the 74 year old quickly bounced back and told Americans, “Don’t let it dominate you. Don’t let it take over your lives.”
But at some point, Trump fully embraced the vaccine charade. Not only did he embrace it, he believed it to be of such critical importance he established the farce that was "Operation Warp Speed." This truly warped endeavour was based on the reality-defying premise that the usual drug development process - and the many years required to properly establish safety and efficacy - could somehow magically be condensed into a few months.
On 2 March 2020, the White House held a roundtable convened by Trump aimed at speeding the development of a COVID vaccine. As CNN reporters noted, "it almost felt like an episode of 'Shark Tank.'"
One by one, vaccine developers pitched their product. John Shiver, the head of R&D for Sanofi Pasteur vaccines said he could have a product ready for the clinic in a year - perhaps a vaccine for the public in as "few as several years."
Trump seemed unmoved. "Right. OK. Thank you very much," he said.
Next was Lenny Schleifer, the founder and CEO of Regeneron, who talked of producing 200,000 vaccine doses per month from his factory, starting in August, "if all goes well."
This got Trump's attention. He leaned over the table and interrupted mid-pitch. "So that process would be faster than John's?" he asked, pointing at Shiver.
"It would be," Schleifer said, adding that the process could take "weeks to months."
The next CEO was Bancel. He glanced across the table at Fauci, and made a point of mentioning he was "very proud to [already] be working with the US government" and "Dr. Fauci's team at the NIH." Bancel went on to say he needed just "a few months" to start Phase Two of the three-phase clinical process that often takes more than a decade.
Trump, noted CNN, seemed to tune out everything but the talk of time.
"So you're talking over the next few months, you think you could have a vaccine?" he asked.
"Correct. Correct," Bancel said, then added, "with phase two," after he noted Fauci shifting in his chair across the table. Fauci then interjected for Trump's benefit: "You won't have a vaccine. You'll have a vaccine to go into testing."
https://anthonycolpo.com/the-disturbing-truth-about-moderna-and-its-mrna-covid-19-vaccine-part-1/trump-whitehouse-vaccine-roundtable/
The very next day, the FDA green-lit Moderna's drug for trial, making it the first COVID vaccine candidate to advance to the first phase of federally-funded clinical study.
Again, this was quite a feat, considering Moderna had never brought a product to market, or gotten any of its nine or so vaccine candidates approved for use by the FDA. It had also never brought a product to the third and final phase of a clinical trial.
But Trump and the Whitehouse weren't finished. On 15 May 2020, they officially announced Operation Warp Speed, which had a war chest of $10 billion of taxpayer money on offer for promising vaccine candidates. The figure was later increased to $18 billion in October 2020.
To top it all off, the person appointed to head Operation Warp Speed was none other than Moderna board member, Moncef Slaoui.
With Operation Warp Speed, Trump did three very regrettable things. He lent credibility to the false claim COVID-19 was so deadly it required a vaccine equivalent of the Manhattan Project. He also established a very dangerous precedent, in which any overhyped virus can now be used to justify "emergency use authorization," conveniently allowing new and poorly tested drugs to be rushed to market on false pretences. And by appointing someone who came straight from a vaccine company to lead the whole charade, Trump signaled that blatant conflicts of interest were A-OK in this already regrettable escapade.
To anyone with the requisite intelligence and powers of reason, this is what will go down as Trump's greatest failure - along with his pandering to the heinous Saudi regime and his indifference to the plight of Julian Assange ("I love WikiLeaks," he told listeners during his 2016 campaign).
Interestingly, his overly cosy relationship with the Saudis - which involved turning a blind eye to their murder of a journalist and the horrors in Yemeni - attracted relatively little criticism from Democrats or the mainstream press, as did his terribly misguided Operation Warp Speed. I guess both sides of the political divide understand war and arms sales are good for the economy, and that giving drug companies something to exuberantly hype is good for the stockmarket. As for Assange, no-one in authority likes a pesky whistle-blower, do they?
So that's Moderna: An overpromising, underdelivering company that became the first company to get US federal backing for COVID vaccine development, not because of its successful track record (it does not have one) but because its quick-talking CEO was able to tell Trump what he wanted to hear.
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0035421
"...challenge of mice given any of the vaccines led to occurrence of Th2-type immunopathology suggesting hypersensitivity to SARS-CoV components was induced. Caution in proceeding to application of a SARS-CoV vaccine in humans is indicated."
All the vaccines used in this research experiment in 2012 triggered hypersensitivity of Th2 immunity. Th2 cells are a subset of CD4+ T helper cells hence the name Th2. The results from this study showed as Th2 immunity triggered by the vaccines increased, the body’s defense system was pushed out of balance and this reaction started to cause tissue breakdown in the lung. This, of course, is concerning.
However, the vaccines given in this paper were not the same as the current mRNA vaccines. The challenging virus was, of course, not SARS-CoV-2. The animals did not die of the disease, they were sacrificed. All other statements concerning this paper are opinions.
This woman testified regarding the danger of Pfizer/Moderna mRNA injections.
https://authentictexan.com/doctor-covid-vaccine-dangers-texas/
I wonder why she is outrightly lying and what conspiring she is doing in the harm of others by testifying this.
https://www.peta.org/media/news-releases/peta-statement-pfizer-vaccine-data/
"The message for the U.S. Food and Drug Administration is clear: Improve vaccine research by removing the requirement for lengthy animal trials." This is extremely unscientific and gears toward a whole medical trajectory which is not evidence based science.
Here, Moderna's chief science officee Tal Zak concludes "I don’t think proving this in an animal model is on the critical path to getting this to a clinical trial."
Animal models play a critical role in all vaccine trials as a means to ensure vaccines are effective as well as safe. The kind of animal used is also critical. They must show a similar course of the disease as do humans. For example, standard laboratory mice are not susceptible to Covid-19 infection because they do not have the same ACE2 receptor sites as humans.** In order to use mice they have to be bred to express the human ACE2 receptors. This receptor is where Covid spikes attach in the lungs causing the cytokine storm and respiratory distress.
Two animal models have been developed for Covid 19, mice and macaques (monkeys). Interesting, the Syrian hamster is stated to be the closest match to humans for Covid-19 testing. “The lungs of infected hamsters exhibit the pathological lesions analogous to the COVID-19 patients with pneumonia. Moreover, the nAb response exhibited by the infected hamster demonstrated immunity against the succeeding re-challenge studies. Furthermore, the transfusion of convalescent sera into the naïve hamsters mounted the antibody response and hence hindered the viral replication in the lungs.”**. I included this statement to emphasize the considerations involved in selecting the animals to use in the trials.
The animal models used by Pfizer and Moderna were mice and macaques (monkeys).* Only Pfizer animal studies are being presented today. “SARS-CoV-2 replicates in the upper and lower respiratory tract and causes pulmonary lesions in both rhesus and cynomolgus macaques. Immune responses against SARS-CoV-2 are also similar in both species and equivalent to those reported in milder infections and convalescent human patients.” * Why the Syrian hamster was not used as an animal model is elusive in Covid-19 animal trial literature.
The following data is from a paper posted September 8, 2020, and entitled,
A prefusion SARS-CoV-2 spike RNA vaccine is highly Immunogenic
and prevents lung infection in non-human primates
24 mice and 18 macaques were injected in the Pfizer Animal Trial with BNT162b2.
2-4 year old Male Macaques Trial
6 male macaques were injected with 30 ug of vaccine, 6 were injected with 100 ug of vaccine, and 6 were injected with saline for controls. They were injected twice, 21 days apart. Seven days after Dose 2 the animals were challenged with Sars-Cov 2 virus. Virus neutralization was noted 14 days after the 30 ug dose of vaccine and 7 days after the 100 ug dose of vaccine. The levels of neutralization were 285 for 30 ug dose and 310 for 100 ug dose persisting to Day 56. This level of neutralization was compared to level of neutralization of human convalescent serum of 94 taken 14 days after a positive PCR test in patients ages 18-83. A Th1 immune response was elicited as well as increased CD4 and CD8 cells.
Vaccination of monkeys reached neutralization titers 10 to 18 times higher than seen on a human convalescent human serum panel. The vaccine generated strong Th1 type CD4 and CD8 T-cell responses in both mice and monkeys. This is a different immune response than presented in last week’s paper in which the macaques lungs were diseased using a different RNA vaccine. With the Pfizer vaccine, the lungs of the macaques were fully protected when challenged by Covid-19 virus. Virus was detected in nasal swabs of non-immunized macaques day 1, 3, 6 after they were challenged with the vaccine, versus virus being detected only on day 1 in immunized macaques. None of the macaques became ill with the virus. The conclusion was,” In general, virus-challenged animals showed no clinical signs of significant disease. We conclude that the 2-4 year old male rhesus macaques challenge model is primarily a SARs-CoV-2 infection model and not for Covid-19 disease model.”*
Mice Trial
Mice were immunized with 0.2, 1, or 5 µg or received a buffer control. IgG antibodies developed rapidly at all dose levels in a dose-dependent manner. SARS CoV-2 neutralization increased steadily after immunization to 296 on Day 28 for the 5 µg dose levels in a dose-dependent manner. A high fraction of CD4 and CD8 T-cells, high levels of Th1 cytokines, and low levels of Th2 cytokines were noted in the lymph nodes. Lung changes were not noted. Little mention was made concerning the controls other than B cells were lower in number than in the immunized mice. The mice were not followed after day 28.
For me, what was learned is the Pfizer vaccine did promote efficient immunization in mice and macaques and did not cause disease using these two models having been followed for 28 and 56 days.
One paper summarized its conclusions by stating, “Nevertheless, the assessment of the vaccine dependent immune enhancement cannot be extrapolated from animal models and requires a legitimate survey from stage III human trials or the human challenge studies.” **
The human trials are being done. We do not know the long term effects of mRNA vaccine. Research will be evaluating those long term side effects by 2022 - keeping in mind the usual process is an average of 10 years.
*https://www.biorxiv.org/content/biorxiv/early/2020/09/08/2020.09.08.280818.full.pdf
*https://www.nature.com/articles/s41467-021-21389-9
**https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7423510/?fbclid=IwAR26kBqLnKbUIWr3MAfOcyd27m_pJfbFM3bvJ9sNUZwJJ6blA6MIIdB_Pzw human trials
**https://www.nature.com/articles/s41684-020-0614-1
****Sars-Cov2 protein subunit vaccination elicits potent neutralizing antibody responses
https://www.modernatx.com/sites/default/files/mRNA-1273-P301-Protocol.pdf
https://pfe-pfizercom-d8-prod.s3.amazonaws.com/2020-09/C4591001_Clinical_Protocol.pdf
In spite of there being 0 official safety data for children, there are now being trials conducted.
https://www.nbcnews.com/news/us-news/moderna-begins-study-covid-19-vaccine-kids-n1261190Moderna has admitted that young children are, in essence, test subjects for substances for which long-term safety is unknown. In a stomach-churning report this March which met with no outrage from moral or ethical leaders, Reuters reported matter-of-factly:
“Moderna Inc has begun dosing patients in a mid-to-late stage study of its Covid-19 vaccine, mRNA-1273, in children aged six months to less than 12 years, the company said on Tuesday. The study will assess the safety and effectiveness of two doses of mRNA-1273 given 28 days apart and intends to enroll about 6,750 children in the United States and Canada.”
This is in spite of the fact children have a 99.997% chance of surviving this virus.mRNA agents given to people with autoimmune issues has also been a problem. A December 2020 article in MedPage Today relates:
“A possible concern could be that some mRNA-based vaccine platforms induce potent type I interferon responses, which have been associated not only with inflammation but also potentially with autoimmunity…Thus, identification of individuals at an increased risk of autoimmune reactions before mRNA vaccination may allow reasonable precautions to be taken.”
In December, British health officials of the Medicines and Healthcare products Regulatory Agency, or MHRA, warned people with food allergies not to take the Pfizer–BioNTech COVID-19 experimental vaccine injection. The advice applied to “any person with a history of a significant allergic reaction to a vaccine, medicines or food.”
The health authority warned of “anaphylactoid reactions.”
CBS News reported in December:
“England’s National Health Service warned on Wednesday that people “with a history of a significant allergic reaction to a vaccine, medicine or food” should not be given the COVID-19 vaccine developed by U.S. pharmaceutical giant Pfizer and Germany’s BioTech.”
Yet, incredibly, no pre-screening is done in the present mass mRNA injection roll-out, and rewards like boxes of donuts are handed out to all-comers, no questions asked.
In a February 2021 interview, Dr. Lee Merritt, a member of America’s Frontline Doctors (AFLD,) a savagely attacked contingent of doctors holding that the lockdowns were unnecessary and the present COVID injections are unsafe, said that upon deliberate reinfection after a time with coronaviruses, most mRNA test animals died of sepsis and organ failure (below.)
Underscoring divisions in the medical community, offices such as McGill University’s Office for Science and Society attack Dr. Merritt and AFLD for things such as “a sordid history of attacking Dr. Fauci’s sound scientific advice,” in an insult-filled rant.
Meanwhile, contrary to the FDA’s and Big Tech, Big Media, and Big Pharma assertions that the “Pfizer” and “Moderna” are safe, a University of Pennsylvania Medical Center paper concludes, in December 2020, that:
“Direct evidence on the comparative safety of mRNA vaccines and other vaccines is lacking.”
Just two of the more prominent calls for a halt to mass “vaccinations” (a term the doctors dispute is accurate) are here, and here.
Even before mRNA technology, coronavirus vaccine development has always been problematic.
The biotech industry newsletter Biopharma Dive writes:
“There has never been a vaccine for any coronavirus. And many vaccine developers have based their designs on previous research into other coronaviruses, like SARS or MERS, which share genetic similarities with SARS-CoV-2, but differences as well. Much still remains unknown about the novel coronavirus, and how our bodies respond to infection.”
The UK Independent reported last year:
“A successful vaccine has never been developed for any of the many strains of coronaviruses, due to the nature of the virus itself; and vaccinated people can have a higher chance of serious illness and death when later exposed to another strain of the virus, a phenomenon known as ‘virus interference.’ An earlier SARS vaccine never made it to market because the laboratory animals it was tested on contracted more serious symptoms on re-infection, and most of them died.”
. Robert F. Kennedy Jr., founder of Children’s Health Defense, writes:
“Scientists first attempted to develop coronavirus vaccines after China’s 2002 SARS-CoV outbreak. Teams of US & foreign scientists vaccinated animals with the four most promising vaccines. At first, the experiment seemed successful as all the animals developed a robust antibody response to coronavirus. However, when the scientists exposed the vaccinated animals to the wild virus, the results were horrifying. Vaccinated animals suffered hyper-immune responses including inflammation throughout their bodies, especially in their lungs. Researchers had seen this same “enhanced immune response” during human testing of the failed RSV vaccine tests in the 1960s. Two children died.”
Many doctors and scientists, whose voices have been silenced, see no need for a vaccine at all for a 99.8% survival rate virus, overall, and 96% for people over 70. Former Vice President and Chief Science Officer for Pfizer for 16 years, Dr. Mike Yeadon, says:
“There is absolutely no need for vaccines to extinguish the pandemic. I’ve never heard such nonsense talked about vaccines.”
“You do not vaccinate people who aren’t at risk from a disease. You also don’t set about planning to vaccinate millions of fit and healthy people with a vaccine that hasn’t been extensively tested on human subjects,”
Although it is frequently compared to the Spanish Flu of 1918, in global deaths per capita, COVID nowhere near, and more similar to the 1957 and 1968 flu pandemics, which few in the general population even knew about, and never prompted talk of masks or lockkdowns.
In previous clinical trials since the 1960’s [8] attempts to vaccinate against RSV, [9] Dengue, [10] SARS and MERS, the studies each failed during the animal phase. Cats, ferrets[22], monkeys, and rabbits each and every time experienced Antibody Dependent Enhancement (ADE), also known as pathogenic priming or a cytokine storm. This occurs when the immune system creates an uncontrolled and overwhelming inflammatory response upon being confronted with the pathogen in the real world, and the outcome, tragically, is death. The same immune system overreaction took place in a number of infants in clinical trials who received an attempted RSV shot, as well as some six hundred Filipino children who died following early vaccination against Dengue [11] and it remains a viable concern today. [12]
Autoimmune disease occurs when the body's immune system can't tell the difference between its own cells and foreign cells, and causes the body to attack its normal cells. [13] It has been suggested that "molecular mimicry" may contribute to this problem, with antibodies to SARS-CoV-2 cross-reacting with structurally similar host protein sequences and raising an acute autoimmune response against them. [14]
Scientists have determined that the same spike protein found in SARS viruses are also responsible for the development of the placenta in mammals, including humans, and is therefore an essential prerequisite for a successful pregnancy. If a woman’s body is primed to attack these protein spikes, the immune system may prevent a placenta from being formed, which would render that woman infertile. [15]
Drs Yeadon and Wodarg further explain; “To my knowledge, Pfizer/BioNTech has yet to release any samples of written materials provided to patients, so it is unclear what, if any, information regarding (potential) fertility-specific risks caused by antibodies is included. According to section 10.4.2 of the Pfizer/BioNTech trial protocol, a woman of childbearing potential is eligible to participate if she is not pregnant or breastfeeding, and is using an acceptable contraceptive method as described in the trial protocol during the intervention period (for a minimum of 28 days after the last dose of study intervention). This means that it could take a relatively long time before a noticeable number of cases of post vaccination infertility could be observed.” [16]
We have additionally heard the reports of multiple cases of Bell's Palsy in both trials [17] and administration, numerous cases of anaphylaxis shock even when no previous allergies were detected, as well as several announced incidents of “false positive” HIV tests. [18]
The remaining elephant in the room is that of the greatest unknown, of tampering with the human genome. There is much we have yet to comprehend of the complexity of the human body and immune system. Science has gotten it wrong many times before, having made assumptions about its ability to exert its dominance over nature. It is still and always nature which has the final say. In the human genome project they tried genetic engineering by changing a singular gene which they believed was the defect in the genetic process. Unexpectedly, instead of correcting, it caused a domino effect of uncontrolled regulation onto multiple other genes.
Of the media press release of 95% efficacy taken as gospel and repeated as fact, Peter Doshi of the British Medical Journal posits whether the study trials were designed too poorly not to fail. With 3,410 total cases of suspected, but unconfirmed COVID 19 in the overall study population accounted for makes a relative risk reduction of 19%, far below the 50% required for emergency use authorization. [19]
Pfiizer, Moderna, Dr Anthony Fauci and Dr Soumya Swaminathan, the WHO’s chief scientist, have made it abundantly clear that the novel mRNA strand entering the cell is not intended to stop transmission but rather as a treatment. However, were we at long last permitted to hold public discourse on the profoundly viable and formerly ubiquitous treatments such as Ivermectin, [20] for one example, and were these treatments not denied us both in access and scientific data but disseminated to the global community, we might not have had need for an emergency use technology at all.
If this experiment does prove to cause any or combination of these problems in a year’s time or a few more and has already been administered to billions worldwide it will be too late. It cannot be removed and it cannot be turned off, it has been irretrievably unleashed into the cellular system. And there is not a government in the world nor the manufacturer himself who will be held accountable if you find yourself come to grave harm. [21]
In a multitude of monumental changes that have taken place over the course of the last year the one thing that has remained consistent is that the mortal risk a Covid-19 infection poses is, with exception, to those above 65 years or with comorbidity. There is not in existence a reasonable scientific or medical indication to inject an experimental technology forever into the veins of anyone outside that narrow group. I argue that to do so it is a reckless and cynical display of disregard for human life and well being in the perverted name of saving a particular few.
We claim an unbridled love of science and yet we are missing the crater sized gaps in reason. A tremendous risk of known and “known unknown” issues is considered against the singular benefit to avert symptoms in questionable potential at best. Tested on an uninformed populace, this is not a flag for public health. The use of the word “vaccine” and the magic bullet it has come to represent confounds the discussion as does its expeditious administration alongside an exponentially changing world. The brevity with which this technology was so recently produced is long forgotten and I, with many others, face the sobering fact that with a now live totalitarian Green Passport initiative, must choose which of my freedoms to concede, the loss of my self determination or my autonomy of body itself.
[1] Sones M (2021) Is Israel a Pfizer test subject?, Arutz Sheva, Accessed on the 12th January from /News/News.aspx/294410
[2] Holmes O (2021) Netanyahu touts Pfizer deal as 20% of Israelis get Covid jab, The Guardian, accessed on the 12th January from https://www.theguardian.com/world/2021/jan/10/netanyahu-touts-pfizer-deal-after-20-of-israelis-get-covid-jab
[3] Central Bureau of Statistics, Population - Statistical Abstract of Israel 2020 - No.71, 2.3 Population, by Population Group, Religion, Sex and Age, accessed on the 12th January 2021 from https://www.cbs.gov.il/en/publications/Pages/2020/Population-Statistical-Abstract-of-Israel-2020-No-71.aspx
[4] Batito E (2020) Controversy erupts around Health Ministry plan to vaccinate on Shabbat, Jerusalem Post, Accessed on the 12th January 2021 from https://www.jpost.com/israel-news/controversy-erupts-around-health-ministry-plan-to-vaccinate-on-shabbat-653253
[5] CDC Website, Vaccines & Immunizations, Immunization: The Basics accessed on the 12th January from https://www.cdc.gov/vaccines/vac-gen/imz-basics.htm
[6] US Food and Drug Administration Website, Medical Device Overview, accessed on the 12th January from https://www.fda.gov/industry/regulated-products/medical-device-overview#What%20is%20a%20medical%20device
[7] CDC Website (2020) Understanding mRNA COVID-19 Vaccines, accessed on the 12th January 2021 from https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/mRNA.html
[8] Su, S., Du, L. & Jiang, S. Learning from the past: development of safe and effective COVID-19 vaccines. Nat Rev Microbiol (2020). https://doi.org/10.1038/s41579-020-00462-y
[9] World Health Organisation Website, Standardization of Respiratory Syncytial Virus (RSV) vaccines, accessed on the 12th January 2021 from https://www.who.int/biologicals/areas/vaccines/RSV/en/
[10] Trial Site News (2020) Philippine Dengue Vaccine Criminal Indictments Includes President of Sanofi Pasteur & their FDA, accessed on the 12th January 2021 from https://trialsitenews.com/philippine-dengue-vaccine-criminal-indictments-includes-president-of-sanofi-pasteur-their-fda/
[11] Trial Site News (2020)
Philippine Dengue Vaccine Criminal Indictments Includes President of Sanofi Pasteur & their FDA, accessed on the 12th January from https://trialsitenews.com/philippine-dengue-vaccine-criminal-indictments-includes-president-of-sanofi-pasteur-their-fda/
[12] Trial Site News (2020) Philippine Dengue Vaccine Criminal Indictments Includes President of Sanofi Pasteur & their FDA, accessed on the 12th January 2021 from https://trialsitenews.com/philippine-dengue-vaccine-criminal-indictments-includes-president-of-sanofi-pasteur-their-fda/
[13] John Hopkins Medicine Website, What Are Common Symptoms of Autoimmune Disease?, Accessed on the 12th January 2021 from https://www.hopkinsmedicine.org/health/wellness-and-prevention/what-are-common-symptoms-of-autoimmune-disease
[14] White S (2020) Rapid Response: Could COVID-19 mRNA vaccines cause autoimmune diseases?, Letter to the British Medical Journal, accessed on the 13th January 2020 from https://www.bmj.com/content/371/bmj.m4347/rr-6 White S (2020) Rapid Response: Could COVID-19 mRNA vaccines cause autoimmune diseases?, Letter to the British Medical Journal, accessed on the 13th January 2020 from https://www.bmj.com/content/371/bmj.m4347/rr-6
[15] Petition from Dr Wolfgang Wodarg and Co Petition from Dr. Michael Yeadon to the European Medical Association, Administrative/Regulatory Stay Of Action on the December 1st 2020, page 5, accessed on the 12th January from https://dryburgh.com/wp-content/uploads/2020/12/Wodarg_Yeadon_EMA_Petition_Pfizer_Trial_FINAL_01DEC2020_signed_with_Exhibits_geschwarzt.pdf
[16] Petition from Dr Wolfgang Wodarg and Co Petition from Dr. Michael Yeadon to the European Medical Association, Administrative/Regulatory Stay Of Action on the December 1st 2020, Page 5, accessed on the 12th January from https://dryburgh.com/wp-content/uploads/2020/12/Wodarg_Yeadon_EMA_Petition_Pfizer_Trial_FINAL_01DEC2020_signed_with_Exhibits_geschwarzt.pdf
[17] FDA Briefing Document, (2020) Vaccines and Related Biological Products Advisory Committee Meeting December 10, 2020, Page 38 and 43, accessed on the 12th January 2021 from https://www.fda.gov/media/144245/download
[18] Rettner R (2020) Why an Australian COVID-19 vaccine caused false-positive HIV test, Live Science, accessed on the 12th January from https://www.livescience.com/australia-covid-19-vaccine-false-positive-hiv-tests.html
[19] Doshi P (2021) Peter Doshi: Pfizer and Moderna’s “95% effective” vaccines—we need more details and the raw data, British Medical Journal, accessed on the 13th January 2021 from https://blogs.bmj.com/bmj/2021/01/04/peter-doshi-pfizer-and-modernas-95-effective-vaccines-we-need-more-details-and-the-raw-data/
[20] Kory, P., MD, Meduri, G. U., MD, Iglesias, J., Varon, J., Berkowitz, K., MD, Kornfeld, H., MD, Marik, P. E. (2020, November 13). Review of the Emerging Evidence Demonstrating the Efficacy of Ivermectin in the Prophylaxis and Treatment of COVID-19. https://doi.org/10.31219/osf.io/wx3zn
[21] Sigalos M (2020) You can’t sue Pfizer or Moderna if you have severe Covid vaccine side effects. The government likely won't compensate you for damages either, CNBC, accessed on the 12th January from https://www.cnbc.com/2020/12/16/covid-vaccine-side-effects-compensation-lawsuit.html?fbclid=IwAR0iLWosxJrjEVIP3v_W0PuRPdMmrFnZ-tgFNT8H9D4O1nEWde5PMQjkuhA
[22] https://journals.asm.org/doi/full/10.1128/JVI.78.22.12672-12676.2004Suspicious events
It seems Albert Bourla, the CEO of Pfizer, doesn’t share the confidence of his own claims. On the day his company issued its press release on the proposed vaccine trials, he sold 62% of his stock in Pfizer, making millions profit in the deal. He made the sell order in a special option in August so it would not appear as “insider selling”, however he also timed it just after the US elections and the mainstream media illegitimately declared Joe Biden President-elect. It seems from appearances that Bourla had a pretty clear conflict of interest in the timing of his press release on the same day.Bourla lied and denied to press that his company had received any funds from the Trump Administration to develop the vaccine when it came out they contracted in summer to deliver 100 million doses to the US Government. Further adding to the suspect actions of Pfized was the fact the company first informed the team of Joe biden rather than the relevant US government agencies.
But this is far from the only thing alarming about the much-hyped Pfizer announcement.
The German Partner
Pfizer, famous for its Viagra and other drugs, has partnered with a small Mainz, Germany company, BioNTech, which has developed the radical mRNA technique used to produce the new corona vaccine. BioNTech was only founded in 2008. BioNTech signed an agreement with the Bill & Melinda Gates Foundation in September, 2019, just before announcement in Wuhan China of the Novel Coronavirus and just before BioNTech made its stock market debut. The agreement involved cooperation on developing new mRNA techniques to treat cancer and HIV. Curiously that press release, “The Gates Foundation sees BioNTech potential to ‘dramatically reduce global HIV and tuberculosis’” 05. September 2019, has now been deleted.
BioNTech also has an agreement with one of the largest drug producers in China, Shanghai Fosun Pharmaceutical Co., Ltd (“Fosun Pharma”) to develop a version of its mRNA vaccine for novel coronavirus for the Chinese market. Ai-Min Hui, President of Global R&D of Fosun Pharma said in an August statement, “Dosing the first Chinese subject with BNT162b1 marks a milestone of the global co-development program in China. We are closely working with BioNTech and regulatory authorities to evaluate the safety and efficacy of BNT162b1 and other mRNA vaccine candidates…”
This means that the same German biotech company is behind the covid vaccines being rushed out in China as well as the USA and EU. The vaccine is being rushed through to eventual approval in an alarmingly short time.
Both US and EU authorities and presumably also Chinese, waived the standard animal tests using ferrets or mice and have gone straight to human “guinea pigs.” Human tests began in late July and early August. Three months is unheard of for testing a new vaccine. Several years is the norm. Because of the degree of global panic engendered by WHO over the coronavirus, caution is thrown to the wind. Vaccine makers all have legal indemnity, meaning they can’t be sued if people die or are maimed from the new vaccine. But the most alarming fact about the new Pfizer-BioNTech gene edited vaccine is that the gene edited mRNA for human vaccine application has never before been approved. Notably, two year peer reviewed tests with mice fed genetically modified corn sprayed with Monsanto glyphosate-rich Roundup first showed cancer tumors after nine months as well as liver and other organ damage. Earlier Monsanto company tests ended at three months and claimed no harm. A similar situation exists with the gene edited mRNA vaccines that are being rushed out after less than 90 days human tests.
“Explicitly experimental”
Dr. Michael Yeadon replied in a recent public social media comment to a colleague in the UK, “All vaccines against the SARS-COV-2 virus are by definition novel. No candidate vaccine has been… in development for more than a few months.” Yeadon then went on to declare, “If any such vaccine is approved for use under any circumstances that are not EXPLICITLY experimental, I believe that recipients are being misled to a criminal extent. This is because there are precisely zero human volunteers for…whom there could possibly be more than a few months past-dose safety information.”
Yeadon is well qualified to make the critique. As he notes in the comment, “I have a degree in Biochemistry & Toxicology & a research based PhD in pharmacology. I have spent 32 years working in pharmaceutical R&D, mostly in new medicines for disorders of lung & skin. I was a VP at Pfizer & CEO…. of a biotech I founded (Ziarco – acquired by Novartis). I’m knowledgeable about new medicine R&D.” He was formerly with Pfizer at a very senior level.
Human guinea pigs?
The Pfizer-BioNTech vaccine is experimental and far from guaranteed safe, despite the fact that Pfizer, the EU and the notorious Dr Tony Fauci seem ready to roll it out even before year end to hundreds of millions of humans.
The experimental technology is based on a rather new gene manipulation known as gene editing. In a major article in the 2018 New York Council on Foreign Relations magazine, Foreign Affairs, Bill Gates effusively promoted the novel gene editing CRISPR technology as being able to “transform global development.” He noted that his Gates Foundation had been financing gene editing developments for vaccines and other applications for a decade.
But is the technology for breaking and splicing of human genes so absolutely safe that it is worth risking on a novel experimental vaccine never before used on humans? Contrary to what Bill Gates claims, the scientific answer is no, it is not proven so safe.
In a peer reviewed article in the October, 2020 journal Trends in Genetics, the authors conclude that “the range of possible molecular events resulting from genome editing has been underestimated and the technology remains unpredictable on, and away from, the target locus.”
Dr. Romeo Quijano, retired professor of Pharmacology and Toxicology at the College of Medicine, University of the Philippines Manila, noted some of the dangers of the experimental gene editing when applied to human vaccines. Quijano warns of, “the danger that the vaccine might actually “enhance” the pathogenicity of the virus, or make it more aggressive possibly due to antibody-dependent enhancement (ADE), as what happened with previous studies on test vaccines in animals. If that should happen in a major human trial the outcome could be disastrous. This serious adverse effect may not even be detected by a clinical trial especially in highly biased clinical trials laden with conflicts of interest involving vaccine companies. Even when a serious adverse event is detected, this is usually swept under the rug.” He cites the case of another Gates mRNA vaccine candidate, Moderna, where “three of the 15 human experimental subjects in the high dose group suffered serious and medically significant symptoms. Moderna, however, concluded that the vaccine was “generally safe and well tolerated,” which the corporate-dominated media dutifully reported, covering-up the real danger…”
He notes, “Exogenous mRNA is inherently immune-stimulatory, and this feature of mRNA could be beneficial or detrimental. It may provide adjuvant activity and it may inhibit antigen expression and negatively affect the immune response. The paradoxical effects of innate immune sensing on different formats of mRNA vaccines are incompletely understood.” Quijano adds, “A mRNA-based vaccine could also induce potent type I interferon responses, which have been associated not only with inflammation but also potentially with autoimmunity… and may promote blood coagulation and pathological thrombus formation.”
Quijano writes in the extensively documented article, “among other dangers, the virus-vectored vaccines could undergo recombination with naturally occurring viruses and produce hybrid viruses that could have undesirable properties affecting transmission or virulence. The…possible outcomes of recombination are practically impossible to quantify accurately given existing tools and knowledge. The risks, however, are real, as exemplified by the emergence of mutant types of viruses, enhanced pathogenicity and unexpected serious adverse events (including death) following haphazard mass vaccination campaigns and previous failed attempts to develop chimeric vaccines using genetic engineering technology.”
Bill Gates, the mRNA vaccine makers including Pfizer/BioNTech and Moderna, and their close allies such as Dr. Tony Fauci of the NIAID are clearly playing fast and loose with human lives in their rush to get these experimental vaccines into our bodies. Notably, the same Dr. Fauci and his NIAID owns the patent on a vaccine for dengue fever known as Dengvaxia, marketed by Sanofi-Pasteur and promoted as an “essential” vaccine by Tedros’ WHO since 2016. Robert F. Kennedy jr. noted that Fauci and NIAID “knew from the clinical trials that there was a problem with paradoxical immune response,” but they gave it to several hundred thousand Filipino kids anyway. It was estimated that as many as 600 vaccinated children died before the government stopped the vaccinations.
Clearly the well-established Precautionary Principle–if in serious doubt, don’t– is being ignored by Fauci, Pfizer/BioNTech and others in rushing to approve the new mRNA vaccine for coronavirus. Messenger RNA technology has yet to produce an approved medicine, let alone a vaccine.
Contrary to the manufacturer’s claim, the mRNA nanoparticles do not remain at the injection site, but are sometimes found in high concentrations in organs, especially in the ovaries in females. The representative of the ministry was asked: “Does the Federal Ministry of Health have similar data for Germany, and if so, how do you rate them?”
The spokesperson responded: “We have four vaccines in Germany that have been approved by the EMA with the corresponding data that have been submitted for them. BioNTech/Pfizer’s vaccine is one of those four vaccines. I would leave it at that.”
The journalist persisted: “My question related to the fact that at least from these data from the Japanese approval authority it is clear that these mRNA nanoparticles do not remain at the puncture site, but were found in high concentrations in the organs. The federal government will certainly also have corresponding data on animal experiments with the vaccine in Germany. Has this phenomenon also been observed?”
But the spokesperson would not comment on these explosive findings: “I cannot comment on what the Japanese regulatory authority has said here. I can tell you that this vaccine has been tested by the EMA and has received regular approval. Since it has this approval, it can be used in Germany as well as in all other EU countries.”
Not only in Israel, but also in the US, several cases are currently being investigated in which vaccinated people developed myocarditis after vaccination with the BioNTech/Pfizer vaccine. According to the responsible health authorities, younger people and men in particular are more likely to be affected than women. But younger people are apparently not the only people who have died after the Corona vaccinations with the BioNTech/Pfizer preparation: A Norwegian committee of health experts has now found that vaccination with the BioNTech/Pfizer vaccine was also “likely” responsible for the deaths of elderly nursing home residents.
As of May 18, 2021, 155 deaths were reported in Norway after vaccination with BioNTech/Pfizer. In most cases, elderly nursing home residents were affected, showing a risk that frail people will die prematurely as a result of the vaccination.
A study from Nature Neuroscience showed that the S1 spike protein of SARS-CoV-2 crosses the blood–brain barrier in mice, causing damage to the cardiovascular and central nervous systems. The spike protein ended up in the peripheral tissues – thus SARS-CoV-2 RNA was recovered from cerebrospinal fluid.
The study showed that these new spike proteins exploit angiotensin-converting enzyme 2 (ACE2), allowing for increased intake of spike proteins into the lungs and specifically to the brain. This is how SARS-CoV-2 manifests in the central nervous system, which include changes to taste and smell, headaches, twitching, seizures, confusion, vision impairment, nerve pain, dizziness, impaired consciousness, nausea, hemiplegia, ataxia, stroke and cerebral hemorrhage.
Spike proteins readily cross the blood-brain barrier through a process called adsorptive transcytosis. Inflammation notably increases spike protein uptake in the brain and lungs. And when the animals were induced with inflammation, the intravenously-administered spike proteins entered the brain more readily.
This is the same spike proteins that human cells now translate, synthesize and replicate using the genetic instructions provided by new mRNA vaccines and adenovirus-vectored vaccines, which is being mass produced to subvert the natural genetic template of protein synthesis.
Canadian virologist Byram Bridle, believes anti-Covid vaccines are directly responsible for cardiovascular injury and death as proposed by the first-of-its-kind “biodistribution” study from Japan showing that even when injected in muscle tissue in the arm, the mRNA (messenger RNA) injections from Moderna and Pfizer/BioNTech cause the production of spike proteins.
“If you inject the ‘purified’ spike protein into the blood … [there is] all kinds of damage to the cardiovascular system, it can cross the blood-brain barrier and cause damage to the brain,” said Bridle. “We thought the spike protein was a great target antigen, we never knew the spike protein itself was a toxin and was a pathogenic protein. So by vaccinating people we are inadvertently inoculating them with a toxin.
“It’s the first time ever scientists have been privy to seeing where these messenger RNA [mRNA] vaccines go after vaccination. Is it a safe assumption that it stays in the shoulder muscle? The short answer is: absolutely not. It’s very disconcerting,” he warned.
Stephanie Seneff, a senior research scientist at Massachusetts Institute of Technology, told LifeSiteNews: “The results of this leaked Pfizer study tracing the biodistribution of the vaccine mRNA are not surprising, but the implications are terrifying.”
While controversial gain-of-function research on Coronaviruses was banned in the US in 2004, it has continued in other countries. Since Coronavirus gain-of-function research began, three new Coronaviruses have emerged. SARS-CoV-1 in 2003; MERS-CoV in 2012; and the current SARS-CoV-2, for which so-called mass-produced vaccines were rolled out globally almost instantly.
New documents obtained by TrialSite News suggest routine quality testing issues were overlooked in the rush to authorize use of the Pfizer/BioNTech COVID vaccine, and that U.S. and other governments are conducting a massive vaccination program with an incompletely characterized experimental vaccine.
Regulatory documents revealed Pfizer didn’t thoroughly examine biodistribution and pharmacokinetics issues relating to its vaccine before submitting the vaccine to the European Medicines Agency (EMA) for review.
In fact, in key studies — called biodistribution studies, which are designed to test where an injected compound travels in the body, and which tissues or organs it accumulates in — Pfizer did not use the commercial vaccine (BNT162b2) but instead relied on a “surrogate” mRNA that produced the luciferase protein.
According to TrialSite News, the EMA reviewers shared this explicit admission: “No traditional pharmacokinetic or biodistribution studies have been performed with the vaccine candidate BNT162b2.”
Pharmacokinetics refers to the study of what the body does with a drug and the drug’s movement throughout the body — the time course of its absorption, bioavailability, distribution, metabolism and excretion.
Regulatory documents also show Pfizer did not follow industry-standard quality management practices during preclinical toxicology studies of its vaccine, as key studies did not meet good laboratory practice (GLP).
Good laboratory practice or GLP is a set of principles intended to assure the quality and integrity of non-clinical laboratory studies used as the basis for research or marketing permits for products regulated by government agencies. The term GLP is most commonly associated with the pharmaceutical industry and the required non-clinical animal testing that must be performed prior to approval of new drug products.
“The implications of these findings are that Pfizer was trying to accelerate the vaccine development timeline based on the pressures of the pandemic,” said TrialSite founder and CEO Daniel O’Connor. “The challenge is that the processes, such as Good Laboratory Practices, are of paramount importance for quality and ultimately for patient safety. If such important steps are skipped, the risk-benefit analysis would need to be compelling.”
O’Connor pointed to the example of generic repurposed drugs that when under evaluation, even if they are approved, must go through “ever more studies to prove their worth.” Yet in the case of the Pfizer vaccine, O’Connor said, “Pfizer was given more discretion even with a radically new life science-based technology.”
According to TrialSite News, it’s standard practice for the EMA to disclose its assessment of investigational new drug submissions. In the case of Pfizer’s vaccine, the EMA assessment included a summary of the agency’s evaluation of the non-clinical vaccine distribution studies reported to EMA by Pfizer — but the EMA did not disclose the results of Pfizer’s biodistribution studies in its public EMA summary.
Studies submitted to the EMA were carried out using two methods: use of mRNA that produces the luciferase protein and use of a radioactive label to mark the mRNA.
The studies revealed the majority of radioactivity initially remained near the injection site. But within hours, a subset of the stabilized mRNA-containing particles became widely distributed throughout the bodies of test animals.
Rapporteur Filip Josephson, (a person appointed by an organization to report on the proceedings of its meetings) and Co-Rapporteur Jean-Michael Race suggested Pfizer used “a qualified LC-MS/MS method to support quantitation of the two novel LNP excipients” and “the bioanalysis methods appear to be adequately characterized and validated for use in the GLP studies.”
However, the studies performed and submitted by Pfizer were non-GLP.
Additionally, the EMA document states, “Biodistribution: Several literature reports indicate that LNP-formulated RNAs can distribute rather nonspecifically to several organs such as spleen, heart, kidney, lung and brain. In line with this, results from the newly transmitted study 185350 indicate a broader biodistribution pattern.”
This EMA observation corresponds with a growing number of adverse events and aligns with data TrialSite obtained through FOIA showing concentrations of LNP-formulated RNAs in the spleen, ovaries, other tissues and organs.
TrialSite news contacted Dr. Robert W. Malone, the original inventor of mRNA vaccine technology and a senior regulatory specialist who serves as president of a prestigious European association who wished to remain anonymous.
When asked to review and comment on the EMA assessment, Malone noted normal pharmacokinetic and pharmaco-toxicology studies had not been performed before EUA authorization for the product.
“I was particularly surprised that the dossier of regulatory documents indicates allowance for use in humans based on non-GLP PK and Tox studies relying on formulations which are significantly different from the final vaccine,“ Malone said.
After completing a review, TrialSite’s other source noted the following:
“A quick review the Toxicology Section (2.3.3) of the European Medicines Agency (EMA) Assessment Report on Comirnaty (COVID-19 mRNA vaccine) issued on 19 February 2021, raises concerns about data applicability of preclinical study findings to clinical use:
“To determine the biodistribution of the LNP-formulated modified mRNA (modRNA), the applicant did study distribution of the modRNA in two different non-GLP studies, in mice and rats, and determined the biodistribution of a surrogate luciferase modRNA.
“Thus, one might question the validity and applicability of non-GLP studies conducted using a variant of the subject mRNA vaccine.
“In addition, no genotoxicity data were provided to EMA.”
According to official government accounts, minimal risk is associated with COVID vaccines when compared to the risks of COVID infection. This belief forms the basis of the U.S. Food and Drug Administration’s Emergency Use Authorization approval, which is based on a risk-benefit analysis.
However, a search in the Centers for Disease Control and Prevention’s Vaccine Adverse Events Reporting System (VAERS) revealed 294,801 reports of adverse events following COVID vaccines, including 5,165 deaths and 25,359 serious injuries between Dec. 14, 2020 and May 28, 2021.
Though the U.S. government argues none of the deaths have been formally linked to COVID vaccines and the reported adverse event risk is low, the discovery of these documents and associated information may alter the risk-benefit assessment underlying the EUA decision, TrialSite News reported.
As The Defender and TrialSite News reported, documents obtained by scientists through the Freedom of Information Act (FOIA) revealed pre-clinical studies showing the active part of the vaccine (mRNA-lipid nanoparticles) — which produce the spike protein — did not stay at the injection site and surrounding lymphoid tissue as scientists originally theorized, but spread widely throughout the body and accumulated in various organs, including the ovaries and spleen.
Research suggests this could lead to the production of spike protein in unintended places, including the brain, ovaries and speen, which may cause the immune system to attack organs and tissues resulting in damage, and raises serious questions about genotoxicity and reproductive toxicity risks associated with the vaccine.
Byram Bridle, a viral immunologist and associate professor at University of Guelph, Ontario, who was awarded a $230,000 grant by the Canadian government last year for research on COVID vaccine development, said he and a group of international scientists filed a request for information from the Japanese regulatory agency to get access to Pfizer’s biodistribution study.
The biodistribution study obtained by Bridle showed the COVID spike protein gets into the blood where it circulates for several days post-vaccination and then accumulates in organs and tissues including the spleen, bone marrow, the liver, adrenal glands and in “quite high concentrations” in the ovaries.
“We made a big mistake. We didn’t realize it until now,” said Bridle. “We thought the spike protein was a great target antigen, we never knew the spike protein itself was a toxin and was a pathogenic protein” that could cause damage in our body if it gets into circulation.
Newly obtained data from the Vaccine Adverse Event Reporting System (VAERS), website shows that unborn children in the womb continue to be adversely affected by COVID 19 vaccines at an alarming rate.
Abortion Free New Mexico has also received expert analysis on the animal trials (published by the European Medicines Agency) for these vaccines that confirm what VAERS reports indicate, that these vaccines are harmful and toxic to unborn babies.
Abortion Free New Mexico has previously reported that none of the COVID 19 vaccines have been approved for pregnant women and are being distributed without full approval from the FDA on an emergency approval basis.
In addition, all four of the vaccines currently being distributed are produced and/or tested with cell lines that originated from an aborted child.
As of May 22, 2021, there are a total of 283 adverse reports in VAERS where the symptom is either “spontaneous abortion” or “fetal death”.
Of these, 9.54% are attributed to J&J/Janssen, 36.75% to Moderna and 53.71% to Pfizer BioNTech.
These cases can be seen in the chart below based on time from vaccination to pregnancy loss.
These events are occurring very close to the time of vaccination, and subsequently falling off as time progresses.
This is highly suggestive of a causative link between the vaccination and the adverse event.
In fact, nearly 30% of these events occurred within 0-2 days after vaccination.
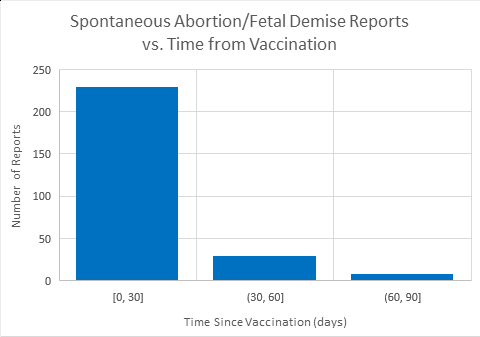
Graph compiled by Abortion Free New Mexico whistleblower. Source.
There are also 18 additional reports of premature birth, premature rupture of membranes and preterm rupture of membranes.
Of these 50% are within the first 0-2 days post-vaccination, and nearly 70% are within the first 10 days post-vaccination.
It is important to note that according to the VAERS website:
“Underreporting” is one of the main limitations of passive surveillance systems, including VAERS. The term, underreporting refers to the fact that VAERS receives reports for only a small fraction of actual adverse events.
VAERS Report Regarding Spontaneous Abortion & Fetal Death processed as of 05/14/2021 .pdf
Tara Shaver, spokeswoman for Abortion Free New Mexico issued the following statement:
All of this data strongly suggests that these experimental ‘vaccines’ are a threat to life in the womb. Some suggest that only 1% of adverse reactions to vaccines are ever reported to VAERS, so the deaths of unborn children could be as high as 28,300.
It’s no secret that Bill Gates, one of the world’s leading population reduction advocates, has stated publicly that vaccines and abortion are the main drivers of his population control agenda.
Unfortunately, we are currently seeing these two pro-death agendas being pushed through extreme political and medical fascism.
Pregnant women should not be encouraged to take these shots and the fact that no one is telling the truth about the dangers posed to their unborn children is unfathomable.
Vaccine Animal Trials Reveal Disturbing Data
According to Abortion Free New Mexico’s whistleblower, who serves on a COVID 19 task force, the U.S. FDA has not released full study details on the animal trials conducted for the COVID 19 vaccines.
However, the European Medicines Agency has and what the animal trials show is that serious birth defects occurred in the rat specimens.
As you will see below, not all was well in the very limited unknown time that the tests were done and the findings do not indicate that they are safe.
These findings are unfortunately not being presented to women when they are offered the vaccines during pregnancy.
Here is the whistleblower’s analysis of this data:
Many online sources claim that the COVID-19 vaccines are “safe” for pregnant mothers.
The CDC website acknowledges that, “experts believe they are unlikely to pose a risk for people who are pregnant…there are currently limited data on the safety of COVID-19 vaccines in pregnant people.”
However, they go on to state that, “studies in animals receiving a Moderna, Pfizer-BioNTech, or J&J/Janssen COVID-19 vaccine during pregnancy found no safety concerns in pregnant animals or their babies”(1) They go on to mention that “early data did not identify any safety concerns for pregnant people who were vaccinated or for their babies.”(1)
The Pfizer factsheets state that pregnant or breastfeeding women should discuss their options with their healthcare providers.(2) Although the U.S. FDA has not released the full study details provided to them for approval of the emergency use authorization (EUA), the European Medicines Agency has.
The full study documents are available at www.ema.europa.eu.
According to a New England Journal of Medicine paper on VAERS and the v-safe surveillance system, since the VAERS system is a passive surveillance system(3), depending on voluntary reporting, “there is probably substantial underreporting of pregnancy and neonatal-specific adverse events.(4)
In addition, the total number of vaccinated pregnant women is not recorded.
The paper also states that, “among pregnancy-specific conditions reported to VAERS after COVID-19 vaccination, miscarriage was the most common.(4)
They also go on to point out that miscarriage was also the most common adverse event reported by pregnant women who received the 2009 H1N1 vaccine.(5)
Besides the miscarriages, the authors state that the data does not indicate safety signals with respect to pregnancy or neonatal outcomes in the third trimester.
In fact, the data shows that 92.3% of the spontaneous abortions occurred before 13 weeks gestation.(4)
According to the reproduction toxicity study on the Pfizer product, performed in pregnant rats: “There was an increase (~2x) of pre-implantation (pregnancy) loss”and,“a very low incidence of gastroschisis, mouth/jaw malformations, right sided aortic arch, and cervical vertebrae abnormalities.”(6)
They claim that these pregnancy reductions are within normal histological ranges, however, they were consistently seen, and are likely statistically significant.Gastroschisis is where the intestines grow outside of the body.
Right-sided aortic arch means the heart has basically formed in the wrong direction (the aortic arch should be on the left side).
Mouth/jaw malformations and cervical vertebrae abnormalities are not described further.
According to the reproduction toxicity study on the Moderna product: “The mRNA-1273-related non-adverse effects were limited to an increase in the number of foetuses with common skeletal variations of 1 or more rib nodules and 1 or more wavy ribs, with no effect on the viability and growth on the F1 generation pups.” and “no vaccine dose was administered during the early organogenesis, to address the direct embryotoxic effect of the components of the vaccine formulation.”(7)
In other words, we don’t know if there would have been teratogenic effects (on development) because the injections were given after the embryo had formed into a fetus.
It goes on to state that, “The overall pregnancy index was numerically lower in mRNA1273 vaccinated female rats (84.1%), compared to control animals (93.2%), but remains within the Test Facility’s historical control range (low range being 75%).”(7) This is still a clear 10% reduction vs the controls.
To say that animal studies found no safety concerns, apparently is a matter of opinion. Based on the data, I disagree with the narrative provided by the CDC.
Unlike traditional vaccines, the Pfizer and Moderna vaccines use nanoparticles to carry instructions on making the COVID 19 viral spike protein to your cells.
The nanoparticles are able to diffuse across your cell membranes indiscriminately. No other vaccines are carried by nanoparticles that are known to cross the blood-brain barrier and literally enter every cell type in our bodies.
Even the COVID-19 virus itself can not do this.
Upon entry, your cells are hijacked to translate the mRNA to spike proteins, which are then anchored to your cell surfaces by an anchor protein also encoded in the mRNA.
Animal studies were also performed to find out where in the body the nanoparticles go.
Regarding the Pfizer product, they report that the nanoparticles were distributed to, “all tissues in the body.” “Over 48 hours distribution was mainly observed to the liver, adrenal glands, spleen and ovaries.”(6)
Additionally they note that, “several literature reports indicate that LNP-formulated RNAs can distribute rather non-specifically to several other organs such as spleen, heart, kidney, lung and brain.”(6)
The Moderna study reported similar findings. They state that “low levels of mRNA could be detected in all examined tissues except the kidney. This included heart, lung, testis and also brain tissues, indicating that the mRNA/LNP crossed the blood brain barrier.”(7)
These findings have troubling implications, not only for pregnancy, but for fertility and, sadly the preservation of every organ system in the body.
If the germ cells, or worse, the neurons, start expressing a viral spike protein, what is to stop the immune system from attacking them?
In response to this expert analysis, Tara Shaver of Abortion Free New Mexico reached the following conclusion.
These animal trial results should be alarming to everyone, especially pregnant women who are being led to believe that the COVID 19 vaccines are safe.
We know that they are experimental and therefore those who take them become part of the experiment.
None of these vaccines have been approved for pregnant women and are only being used on an emergency basis for the rest of the population.
It is dangerous territory to bring innocent, helpless and defenseless unborn children into this human experiment not knowing the exact short and long term outcomes.
The VAERS data clearly shows that hundreds of babies in the womb have died because their moms took these vaccines.
If this wasn't awful enough, have a look at the abortion derived cell lines involvled in the vaccine, all with clear links to the research.
https://lozierinstitute.org/update-covid-19-vaccine-candidates-and-abortion-derived-cell-lines/
https://healthimpactnews.com/2021/20595-dead-1-9-million-injured-50-serious-reported-in-european-unions-database-of-adverse-drug-reactions-for-covid-19-shots/
Comments
Post a Comment